
Table of Contents >> Show >> Hide
- What Is a Pulmonary Embolism?
- Common Pulmonary Embolism Symptoms
- When to Seek Emergency Care
- Why Pulmonary Embolism Happens
- Risk Factors: Who’s More Likely to Get a PE?
- How Doctors Diagnose Pulmonary Embolism
- Treatment: How a Pulmonary Embolism Is Managed
- Recovery: What to Expect After a PE
- Prevention: How to Lower Your Risk
- Frequently Asked Questions
- Conclusion
- Real-World Experiences With Pulmonary Embolism (What People Commonly Report)
- 1) “I thought I was just out of shapeor anxious.”
- 2) “The chest pain felt weirdlike a stitch, not a heart attack.”
- 3) “The leg symptoms were the warning I didn’t connect.”
- 4) “It happened after a ‘perfect storm’ week.”
- 5) “Treatment was less scary once I understood the plan.”
- 6) “Recovery was a marathon, not a sprint.”
A pulmonary embolism (PE) is the medical version of a traffic jam you never want: a blood clot blocks blood flow in the arteries of your lungs.
It’s serious, it can be sudden, and it absolutely deserves quick attention. The good news? PE is also very treatableespecially when it’s caught early.
This guide covers what a pulmonary embolism is, the most common symptoms, who’s at higher risk, how doctors diagnose it, what treatment looks like,
and how to reduce your chances of dealing with one in the first place. (Spoiler: your legs matter more than you think.)
What Is a Pulmonary Embolism?
A pulmonary embolism happens when a clot (or, less commonly, other material) lodges in a lung artery and blocks blood flow.
Most of the time, the clot starts somewhere elsetypically in a deep vein in the leg or pelvis. That original clot is called a deep vein thrombosis (DVT).
When part of that clot breaks off and travels to the lungs, it becomes a PE.
Why is that a problem? Because your lungs are where your blood picks up oxygen.
Blocked blood flow can reduce oxygen levels, strain the right side of the heart, andif the clot is large enoughbecome life-threatening.
Common Pulmonary Embolism Symptoms
PE symptoms can show up suddenly or build over time. Some people have obvious “something is very wrong” symptoms.
Others have milder symptoms that look like anxiety, a pulled muscle, or a bad respiratory day. That’s why PE is often described as a master of disguise.
Most common symptoms
- Shortness of breath (at rest or with activity)
- Chest pain that may feel sharp and can get worse with a deep breath, coughing, or bending
- Fast breathing or feeling like you can’t take a full breath
- Fast heart rate or “my heart is racing” sensation
- Cough (sometimes with blood-tinged mucus)
Symptoms that can happen with more severe PE
- Lightheadedness, near-fainting, or fainting
- Very low blood pressure
- Blue or gray lips/fingertips (sign of low oxygen)
- Confusion or feeling suddenly “out of it”
Important note: PE can sometimes occur without noticeable leg symptoms. So “my leg feels fine” doesn’t automatically mean “my lungs are fine.”
When to Seek Emergency Care
Call emergency services or seek urgent medical care right away if you have:
unexplained shortness of breath, chest pain, fainting, or coughing up blood.
These symptoms don’t always mean PEbut they’re serious enough that it’s safer to get checked immediately.
If you’re thinking, “But I don’t want to overreact,” remember this: your lungs are not the place for a “let’s wait and see” experiment.
Why Pulmonary Embolism Happens
Most pulmonary embolisms come from blood clots formed in deep veins, especially in the legs.
Clots are more likely when blood flow slows down, blood becomes more prone to clotting, or the lining of a vein is irritated or injured.
Doctors often group risk factors into a simple trio:
- Slower blood flow (think long periods sitting still)
- Vein injury (surgery, trauma, inflammation)
- “Stickier” blood (certain conditions or medications that increase clot risk)
Risk Factors: Who’s More Likely to Get a PE?
Anyone can develop a pulmonary embolism, but your odds go up when you have one or more of these risk factors:
Movement and travel factors
- Long periods of immobility (bed rest, hospitalization, long car trips, long flights)
- Limited mobility after surgery or injury
Medical and life factors
- Recent surgery (especially orthopedic surgery like hip or knee procedures)
- Recent trauma or fractures
- Pregnancy and the postpartum period
- Cancer and certain cancer treatments
- Prior history of DVT or PE
- Known clotting disorders (inherited or acquired)
- Smoking (especially when combined with other risks)
- Obesity and older age (risk increases as we age)
- Heart failure and some chronic illnesses
Hormones and medications
- Estrogen-containing birth control
- Hormone therapy with estrogen
Having multiple risk factors at the same time matters. A long flight plus dehydration plus estrogen-containing birth control plus a recent injury?
That’s not “four separate little risks.” That’s a risk stacklike Jenga, but with your circulation.
How Doctors Diagnose Pulmonary Embolism
Because PE symptoms can mimic many other problems (asthma flare, pneumonia, panic attack, heart issues), diagnosis is about combining:
your symptoms, your risk factors, a physical exam, and targeted testing.
Common steps in evaluation
-
Clinical risk assessment: Clinicians often estimate how likely PE is based on symptoms and risk factors.
This helps decide what tests to do next. -
D-dimer blood test: D-dimer can be elevated when the body is forming and breaking down clots.
It’s most useful when the overall suspicion is low to moderate, because a normal result can help rule out PE in many cases. -
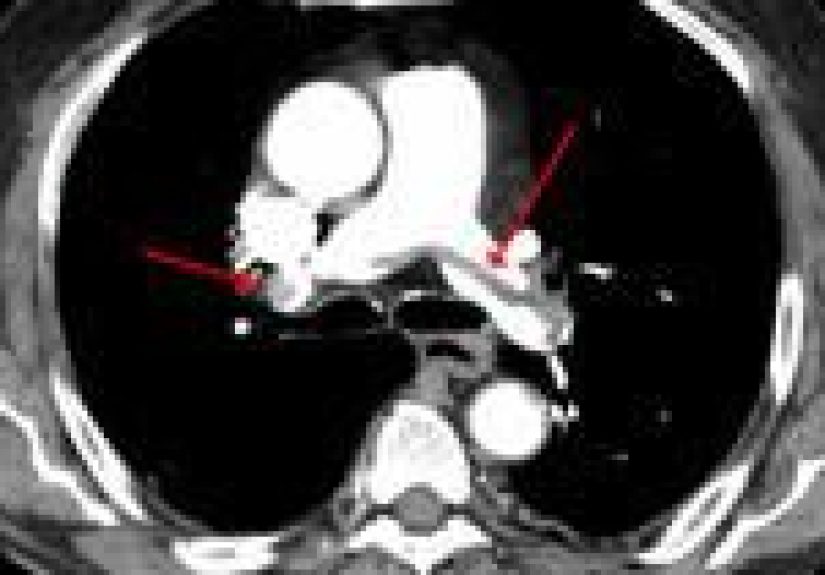
Imaging: The most common imaging test is a CT pulmonary angiography (CTPA), which can show clots in the lung arteries.
In some situationslike certain kidney issues, contrast allergy, or pregnancydoctors may use a ventilation-perfusion (V/Q) scan instead. - Leg ultrasound: If DVT is suspected, an ultrasound of the leg veins may help.
- Heart strain checks: An echocardiogram or blood tests may be used to assess how much strain the clot is putting on the heart.
Diagnosis isn’t about “one perfect test.” It’s about choosing the right tests for the right personfastwithout exposing someone to unnecessary scans.
Treatment: How a Pulmonary Embolism Is Managed
Treatment depends on how big the clot is, how stable the person is, and whether the heart and oxygen levels are affected.
The goal is to stop the clot from getting bigger, prevent new clots, and give the body time to gradually break down the existing clot.
1) Anticoagulants (“blood thinners”)
Anticoagulants are the main treatment for most PEs. Despite the nickname, they don’t actually “thin” your blood.
They reduce your blood’s ability to form new clots and keep existing clots from growing.
Your body then has time to slowly dissolve the clot on its own.
Common anticoagulant options include:
- Direct oral anticoagulants (DOACs) in many cases
- Heparin (unfractionated) or low-molecular-weight heparin in certain situations
- Warfarin for some patients, with monitoring
Treatment length often starts at at least 3 months, but may be longer depending on whether the PE was provoked (like surgery)
or unprovoked (no clear trigger), as well as ongoing risk factors.
2) Clot-busting medications (thrombolysis)
If a PE is large and causing dangerous instability (for example, very low blood pressure or severe heart strain),
doctors may consider thrombolytic medication to dissolve the clot more quickly. This can be lifesaving,
but it also raises bleeding riskso it’s reserved for select, higher-risk situations.
3) Catheter-based or surgical clot removal
In certain severe casesor when thrombolytics aren’t appropriatespecialized teams can use catheter-based techniques to break up
or remove the clot. Rarely, surgery may be needed.
4) Inferior vena cava (IVC) filters (selected cases)
An IVC filter is a device placed in a large vein (the inferior vena cava) to trap clots traveling from the legs before they reach the lungs.
These are typically considered when someone cannot take anticoagulants due to bleeding risk, or in certain complex cases.
They are not a replacement for anticoagulation in most people.
Recovery: What to Expect After a PE
Recovery isn’t always instant. Some people feel better in days; others take weeks or months to fully bounce back.
Fatigue and shortness of breath can linger as the body heals and rebalances.
Follow-up matters
- Medication adherence: Taking anticoagulants as prescribed is crucial.
- Bleeding awareness: Anticoagulants increase bleeding risk, so you’ll usually get safety instructions (and what to do if bleeding happens).
- Symptom monitoring: Worsening shortness of breath, chest pain, or fainting requires urgent evaluation.
Possible complications
- Post-PE symptoms: Some people have ongoing shortness of breath, exercise intolerance, or chest discomfort for a while.
-
Chronic thromboembolic pulmonary hypertension (CTEPH): A rare but serious condition where blood pressure in lung arteries remains high due to chronic obstruction or vessel changes.
Persistent breathlessness after PE is one reason follow-up is important.
Prevention: How to Lower Your Risk
You can’t control every risk factorbut you can reduce the “clot-friendly” conditions that make a DVT (and then a PE) more likely.
Practical prevention habits
- Move regularly: On long trips, stand up, stretch, and walk when possible. Flex your ankles and calves while seated.
- Hydrate: Dehydration can contribute to thicker blood and reduced circulation.
- Know your personal risk: If you’ve had a prior DVT/PE or have major risk factors, ask your clinician what prevention makes sense for travel or surgery.
- After surgery: Follow instructions about early walking, compression devices, and any prescribed preventive medications.
- Don’t ignore leg symptoms: New one-sided leg swelling, pain, warmth, or redness deserves prompt evaluation.
Think of your calves as the “backup pumps” for returning blood to your heartespecially when you’re sitting.
If they’re off-duty for too long, blood can pool. And pooled blood is where clots like to throw parties.
Frequently Asked Questions
Can you have a pulmonary embolism with normal oxygen levels?
Yes. Oxygen levels can be normal early on or with smaller clots. That’s why clinicians focus on the whole picturesymptoms, risk factors, exam findings, and testing.
Is chest pain always severe with PE?
Not always. Some people describe sharp pain with breathing; others describe vague pressure, back pain, or discomfort that comes and goes.
The variability is exactly why unexplained symptomsespecially with risk factorsshould be checked.
Will anticoagulants dissolve the clot?
Anticoagulants usually prevent growth and new clots. Your body does most of the “cleanup” work over time.
In severe cases, clot-dissolving medication or procedures may be used for faster removal.
Conclusion
A pulmonary embolism is a serious blood clot in the lungoften arriving from a DVT in the legand it can be life-threatening without prompt care.
Key symptoms include sudden shortness of breath, chest pain that worsens with breathing, a rapid heartbeat, and sometimes fainting or coughing up blood.
Because PE can mimic other conditions, diagnosis relies on clinical assessment and targeted testing, and treatment often includes anticoagulants
(with advanced therapies reserved for higher-risk cases).
If you remember just one thing: don’t ignore unexplained breathing trouble or chest painespecially if you’ve been immobile, recently had surgery, or have other clot risks.
Quick evaluation can be the difference between a close call and a crisis.
SEO tags (JSON) are provided at the very end of this article.
Real-World Experiences With Pulmonary Embolism (What People Commonly Report)
Everyone’s PE story is different, but certain themes show up again and againespecially the way symptoms can feel “not quite right,”
but not always dramatic enough to scream emergency at first. Below are realistic, experience-based patterns people often describe.
(These are not personal stories from the authorthink of them as composites of common patient experiences shared in clinics and educational resources.)
1) “I thought I was just out of shapeor anxious.”
A surprisingly common experience is subtle shortness of breath that doesn’t match the situation. Someone might notice they’re winded climbing stairs
they normally handle easily, or they feel like they can’t get a satisfying breath while sitting still. Because shortness of breath can also happen with
stress, panic, or lack of sleep, many people chalk it up to anxietyespecially if they’ve been under pressure. A clue that pushes some people toward care
is that the sensation doesn’t resolve with calming down, rest, or typical coping strategies, and it may be paired with a fast heartbeat.
2) “The chest pain felt weirdlike a stitch, not a heart attack.”
Not everyone gets crushing chest pressure. Many people describe a sharp pain that’s worse when they inhale deeply, cough, or laughalmost like a stubborn
side stitch that refuses to leave. Some feel it in the upper back or shoulder area. Because it can mimic a pulled muscle, rib strain, or even reflux,
it’s easy to delay care. People often report that the pain is “breathing-related” more than “movement-related,” which is one reason clinicians take
pleuritic (breath-worsened) pain seriously when other risk factors are present.
3) “The leg symptoms were the warning I didn’t connect.”
Another frequent theme: leg symptoms showed up first, but didn’t seem urgent. One calf looks more swollen than the other, feels warm, or aches like a
charley horse that won’t go away. Some people notice tenderness behind the knee or along the calf. Others have no leg pain at all, which is why PE can
feel so sneaky. Still, when leg symptoms and breathing symptoms appear within days of each other, that pairing is a major red flag.
4) “It happened after a ‘perfect storm’ week.”
Many people can point to a cluster of risks: a long flight or road trip, followed by a busy stretch where they sat more than usual, plus dehydration,
plus a recent illness or minor injury. Others describe it after surgeryespecially when they were moving less during recovery. People dealing with cancer,
pregnancy/postpartum changes, or estrogen-containing medications sometimes learn later that their baseline risk was already higher, and the additional trigger
tipped the balance.
5) “Treatment was less scary once I understood the plan.”
A lot of fear comes from the phrase “blood clot in the lung.” Once treatment starts, many people report relief just knowing there’s a clear plan:
anticoagulants to prevent growth, follow-up to monitor recovery, and education on bleeding precautions. People often say the most practical challenges are
routineremembering doses, navigating medication interactions, and learning when to call the doctor. Over time, confidence grows as breathing improves and
activity becomes easier again.
6) “Recovery was a marathon, not a sprint.”
Some people feel dramatically better within days. Others describe lingering fatigue, shortness of breath with exertion, or a “my body feels cautious” phase
that lasts weeks. It’s common to rebuild activity gradually. Many people find it reassuring to have a follow-up plan, especially if symptoms persist,
because ongoing breathlessness deserves evaluation to rule out complications and to guide rehabilitation.
If these experiences sound familiar and you’re worried, the safest move is to get medical advice promptly.
When it comes to PE, it’s better to feel slightly embarrassed in a waiting room than to be brave at home with a condition that needs treatment.






