
Table of Contents >> Show >> Hide
- What Is Endometrial (Uterine) Cancer?
- Common Symptoms: The Signs You Shouldn’t Ignore
- Risk Factors: Who Is More Likely to Get Endometrial Cancer?
- There’s No Routine ScreeningSo Awareness Matters
- How Endometrial Cancer Is Diagnosed
- Staging, Grading, and Biomarkers: What Those Labels Mean
- Treatment Options: What Care Often Looks Like
- Life After Treatment: Follow-Up, Side Effects, and Getting Back to “You”
- Risk Reduction: What You Can Do (Without Blaming Yourself)
- Questions to Ask Your Clinician
- Experiences People Commonly Describe (A 500-Word Reality Check)
Your uterus is not the type to send push notifications. It doesn’t pop up a banner that says,
“Hey bestie, something’s off.” Instead, it tends to whisperoften through changes like unexpected
bleeding, spotting, or new pelvic symptoms. The good news? Endometrial cancer (the most common type
of uterine cancer) is often found earlier than many other cancers because those “whispers” are hard
to ignore once you know what to listen for.
This guide breaks down what endometrial (uterine) cancer is, who’s at higher risk, common symptoms,
how doctors diagnose and stage it, and what treatment options may look like todayincluding surgery,
radiation, chemotherapy, hormone therapy, and newer immunotherapy approaches. It’s written for real
life: clear, practical, and respectful (with just enough humor to keep things human).
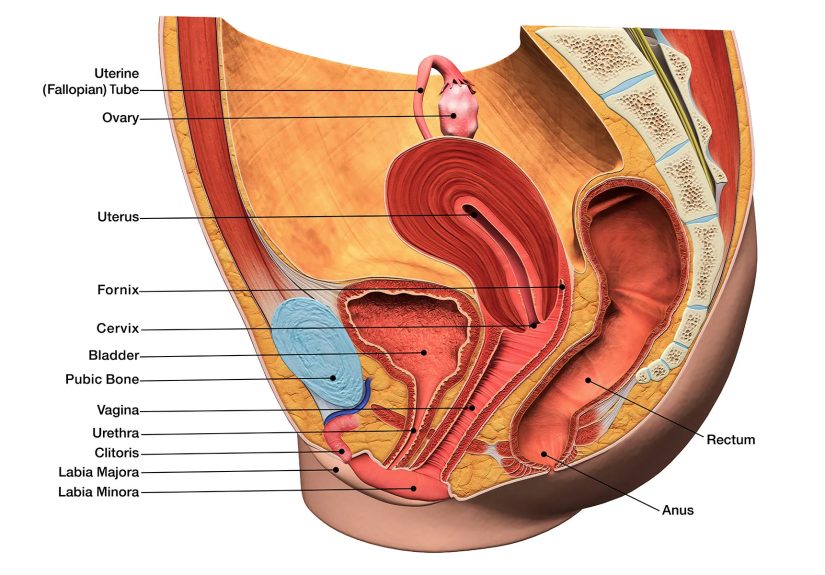
What Is Endometrial (Uterine) Cancer?
“Uterine cancer” is a broad term for cancers that start in the uterus. Most uterine cancers are
endometrial cancer, meaning they begin in the lining of the uterus (the endometrium).
A less common group, uterine sarcomas, start in the muscle or supporting tissues of
the uterus and behave differently.
Endometrial cancer is often discussed in “types.” Many cases are endometrioid (a common subtype),
while otherssuch as serous or clear cellare less common but may be more aggressive. Doctors also
describe tumors by grade (how abnormal cells look under a microscope) and by
stage (how far the cancer has spread).
Why the “Endometrium” Matters
The endometrium responds to hormones, mainly estrogen and progesterone. Over many years, situations
that increase “unopposed estrogen” (estrogen without enough progesterone to balance it) can contribute
to abnormal thickening of the lining and, in some people, cancer development. That’s one reason risk
factors often overlap with hormone patterns and metabolic health.
Common Symptoms: The Signs You Shouldn’t Ignore
The most common early sign is abnormal vaginal bleeding. That can look different
depending on your life stage:
- After menopause: any bleeding or spotting is a “call your clinician” symptom.
- Before menopause: bleeding between periods, unusually heavy periods, or cycles that suddenly change.
- Anytime: unusual watery or blood-tinged discharge, pelvic pain/pressure, or pain during urination (less common).
Important reality check: many non-cancer conditions can cause abnormal bleeding (fibroids, polyps,
hormonal shifts, infections). But endometrial cancer is one of the reasons clinicians take these
symptoms seriouslyespecially after menopausebecause early evaluation can make a big difference.
When to Seek Care Quickly
If you have bleeding after menopause, persistent spotting, or bleeding that’s new and unexplained,
it’s worth scheduling an evaluation promptly. Think of it like a smoke alarm: it doesn’t prove there’s
a fire, but it’s not a sound you ignore and “see how it goes.”
Risk Factors: Who Is More Likely to Get Endometrial Cancer?
Risk factors don’t mean someone will develop endometrial cancer. They simply shift the odds. Many
people diagnosed have only a few risk factorsand some have none that stand out.
Higher-Risk Patterns
- Age: risk increases as people get older; many diagnoses happen around or after menopause.
- Body weight and metabolic health: obesity, insulin resistance, and diabetes are associated with higher risk.
- Unopposed estrogen exposure: estrogen-only hormone therapy (without progesterone) in people with a uterus.
- Irregular ovulation: conditions like polycystic ovary syndrome (PCOS) can be linked to long-term hormone imbalance.
- Tamoxifen: a medication used for breast cancer risk/treatment can slightly increase endometrial cancer risk.
- Family history and inherited syndromes: Lynch syndrome is a key example that raises risk for several cancers, including endometrial cancer.
Protective Factors (Yes, Those Exist)
Some factors appear to lower risk, including long-term use of combined hormonal birth control and
use of progesterone-containing options in appropriate situations. Pregnancy history and breastfeeding
are sometimes discussed as protective in research, but individual risk is complex. If you’re deciding
on hormone therapy or contraception, the best approach is a personalized discussion based on your
medical history.
There’s No Routine ScreeningSo Awareness Matters
Unlike cervical cancer, which has screening options (like the Pap test and HPV testing), there is
no routine screening test for uterine cancer for people without symptoms.
A Pap test does not screen for endometrial cancer. That’s why symptom awarenessespecially
postmenopausal bleedingis such a big deal.
People at higher inherited risk (such as Lynch syndrome) may have specialized surveillance plans.
If multiple relatives have had colon cancer, endometrial cancer, or related cancersespecially at
younger agesask a clinician whether genetic counseling makes sense.
How Endometrial Cancer Is Diagnosed
Diagnosis usually starts with a symptom (most often abnormal bleeding) and proceeds step-by-step.
Clinicians may use a combination of imaging and tissue sampling.
Typical Diagnostic Tools
- Pelvic exam: checks for masses, tenderness, or other causes of symptoms.
- Transvaginal ultrasound (TVUS): often used to evaluate the endometrium, especially after menopause.
- Endometrial biopsy: a small sample of the uterine lining is collected and examined under a microscope.
- D&C (dilation and curettage) or hysteroscopy: used when biopsy isn’t enough or symptoms persist.
- Imaging (CT/MRI/PET in selected cases): helps assess spread and supports treatment planning.
A Common Real-World Example
Imagine someone who has been menopausal for two years and then has spotting. A clinician may start
with a transvaginal ultrasound. If the lining looks thicker than expected or symptoms persist, an
endometrial biopsy is often recommended. If biopsy results are unclearor if there’s concern for a
focal polyp or lesiona hysteroscopy may follow. Each step narrows the “why” behind the bleeding.
Staging, Grading, and Biomarkers: What Those Labels Mean
Once cancer is confirmed, the care team determines how advanced it is. Most endometrial cancers are
staged surgicallymeaning the stage is based on what’s found during surgery and under the microscope.
Stage (Where the Cancer Is)
In general terms, stages run from I to IV:
- Stage I: confined to the uterus.
- Stage II: involves the cervix but hasn’t spread beyond the uterus.
- Stage III: spread to nearby areas (like ovaries, tubes, vagina, or regional lymph nodes).
- Stage IV: spread to the bladder/rectum lining or distant sites.
Staging systems are evolving as molecular testing becomes more common. Some newer staging updates
incorporate biomarkers, but adoption can vary depending on available testing and local practice.
Grade (How the Cells Look)
Grade helps estimate how quickly a tumor might grow and spread. Lower-grade tumors often behave
less aggressively than higher-grade tumors, though every individual case is unique.
Biomarkers and Molecular Testing (The “Precision Medicine” Layer)
More care teams now test tumors for markers that can guide treatmentespecially in higher-risk,
advanced, or recurrent disease. Examples include mismatch repair deficiency (dMMR)/MSI status,
POLE mutations, p53 abnormalities, and sometimes HER2 in certain aggressive subtypes.
The point isn’t to collect fancy acronymsit’s to choose treatments more intelligently.
Treatment Options: What Care Often Looks Like
Treatment depends on stage, tumor type/grade, biomarkers, overall health, and personal goals.
Many people hear “cancer” and imagine one standard plan. Endometrial cancer treatment is more like a
menu: some people need a simple combination, others need a multi-course meal.
Surgery (Often the Foundation)
For many cases, the main treatment is surgery, typically a hysterectomy (removal of
the uterus) plus removal of the fallopian tubes and ovaries (often called BSO). Depending on risk,
the surgeon may also evaluate lymph nodes. In many centers, sentinel lymph node mapping
helps check lymph nodes while reducing the risk of complications compared with more extensive removal.
When possible, minimally invasive approaches (laparoscopic or robotic) can shorten recovery time.
The “best” approach depends on the situation and the surgical team’s expertise.
Radiation Therapy
Radiation may be used after surgery to reduce recurrence risk, or in cases where surgery isn’t the
best option. Two common forms are:
- Vaginal brachytherapy: internal radiation targeting the top of the vagina (often used in select early-stage cases).
- External beam radiation: targets the pelvis and sometimes broader areas depending on risk and spread.
Chemotherapy
Chemotherapy is more common for higher-grade tumors, later stages, or cancers that have spread or
returned. One widely used combination includes carboplatin and paclitaxel. Chemo decisions are
personalizedsome people receive it after surgery; others receive it alongside radiation.
Hormone Therapy (For Certain Tumors)
Some endometrial cancers are hormone-sensitive. In specific situationssuch as selected cases of
early disease where fertility preservation is a goal, or in some advanced/recurrent settingsprogestin-based
therapy or other hormone approaches may be considered. This is highly individualized and requires close follow-up.
Immunotherapy and Targeted Therapy (Newer Options)
In advanced or recurrent endometrial cancer, especially when tumors show certain biomarkers (like dMMR/MSI-H),
immunotherapy can play an important role. For some patients, combinations such as immunotherapy plus other agents
are used based on tumor features and prior treatments. Clinical trials are also a major part of progress here,
and many people ask about them earlynot as a “last resort,” but as another path to strong options.
Life After Treatment: Follow-Up, Side Effects, and Getting Back to “You”
After treatment, follow-up visits often focus on:
- Monitoring for recurrence (symptoms, exams, and imaging when appropriate)
- Managing side effects (fatigue, menopausal symptoms after ovary removal, pelvic changes after radiation)
- Supporting overall health (activity, nutrition, sleep, mental well-being)
Many people are surprised by the emotional whiplash: relief mixed with worry, gratitude mixed with
frustration, and a whole lot of “Wait… now what?” If that’s you, you’re not dramaticyou’re human.
Support groups, counseling, and survivorship programs can help.
Practical Tips That Often Help
- Bring a question list to appointments (and a friend if you want a second set of ears).
- Track symptoms briefly: what’s new, how long, what makes it better/worse.
- Ask about rehab services (pelvic floor physical therapy, nutrition support, fatigue management).
- Don’t “tough it out” aloneside effects are medical issues, not personality tests.
Risk Reduction: What You Can Do (Without Blaming Yourself)
It’s worth saying out loud: cancer is not a moral failing. Still, some steps may help reduce risk
or support overall health:
- Maintaining a weight that supports metabolic health (whatever that means for your body and situation)
- Staying physically active in a sustainable way
- Managing diabetes and blood pressure with your healthcare team
- Using hormone therapy thoughtfullyestrogen alone is generally not recommended for people with a uterus
- Considering genetic counseling if family history suggests inherited risk
The goal isn’t perfection. The goal is stacking small advantages in your favor while staying kind to yourself.
Questions to Ask Your Clinician
If you’re navigating diagnosis or treatment planning, these questions can bring clarity:
- What type and grade of endometrial cancer is this?
- What stage is it, and how was that determined?
- Do I need biomarker or genetic testing (MMR/MSI, POLE, p53, HER2, Lynch syndrome evaluation)?
- Is sentinel lymph node mapping appropriate for me?
- What treatments do you recommendand why this plan over alternatives?
- What side effects should I expect, and what can we do to prevent or treat them?
- Should I consider a second opinion or a clinical trial?
Experiences People Commonly Describe (A 500-Word Reality Check)
Because I’m an AI, I don’t have personal experiencesbut I can share patterns that many patients and caregivers
commonly describe when dealing with endometrial (uterine) cancer. If you’re in this chapter of life, you may
recognize some of these moments. And if you’re supporting someone else, consider this your “what it can feel like”
guide.
First, there’s often a moment of disbelief: “It’s probably nothing.” For many people, the earliest clue is
unexpected spottingespecially after menopause. The symptom itself may be light, even intermittent, which makes
it emotionally easy to postpone care. A common reflection later is, “I’m glad I didn’t ignore it.” Not because
everyone with spotting has cancer (most do not), but because getting evaluated quickly restores controleither
by ruling out something serious or by catching it early.
Then comes the waiting: waiting for appointments, waiting for biopsy results, waiting for a treatment plan.
People describe this as the hardest part because the mind fills silence with worst-case scenarios. Many say it
helped to write down questions in a notebook, bring someone to visits, and ask for explanations in plain English.
(“Can you tell me what you know, what you don’t know yet, and what happens next?” is a surprisingly powerful
sentence.)
Surgery can feel like a finish line and a starting line at the same time. Some people feel relief“Get it out.”
Others grieve what the uterus represents: fertility, identity, or simply the sense that the body has changed.
Recovery stories often include small milestones that deserve real credit: walking a little farther each day,
sleeping through the night, showering without feeling exhausted afterward, laughing without discomfort, and
gradually trusting the body again. Many people are also surprised by the emotional side of recovery: even when
everything goes “well,” the nervous system may stay on high alert for a while.
For those who need radiation or chemotherapy, people often describe learning a new skill set: symptom tracking,
hydration routines, “good days vs. quiet days,” and accepting help without guilt. Caregivers commonly say they
felt most useful when they handled logisticsrides, meals, appointment notesso the patient could spend energy
on healing. And across many stories, one theme repeats: side effects are not something you have to earn or endure.
People who spoke up earlyabout fatigue, nausea, pain, anxiety, sleep, menopausal symptomsoften got better tools
and felt more like themselves sooner.
Finally, survivorship has its own learning curve. Even after treatment, many people describe “scanxiety” and
worry before follow-ups. What helps? A clear follow-up plan, supportive community, and permission to live life
between appointments. If you’re in this space, you’re not expected to be brave 24/7. You’re allowed to be a
whole personmessy feelings included.






