
Table of Contents >> Show >> Hide
- What Is Cervical Cancer?
- Cervical Cancer Symptoms: What to Watch For
- What Causes Cervical Cancer?
- Risk Factors That Make Cervical Cancer More Likely
- How Cervical Cancer Is Diagnosed
- Screening and Prevention: The Best Plot Twist
- Cervical Cancer Treatment: What the Options Look Like
- Side Effects and Recovery: The Part Nobody Should Sugarcoat
- What Prognosis Depends On
- When to See a Doctor
- Real-Life Experiences With Cervical Cancer: What Many Patients Go Through
- Conclusion
Cervical cancer does not usually kick down the door and announce itself with a brass band. In many cases, it starts quietly, develops slowly, and gives people plenty of chances to catch it earlyif they know what to watch for and keep up with screening. That is the frustrating part and the hopeful part. Frustrating, because early cervical cancer may cause no symptoms at all. Hopeful, because this is one of the more preventable and treatable cancers when it is found early.
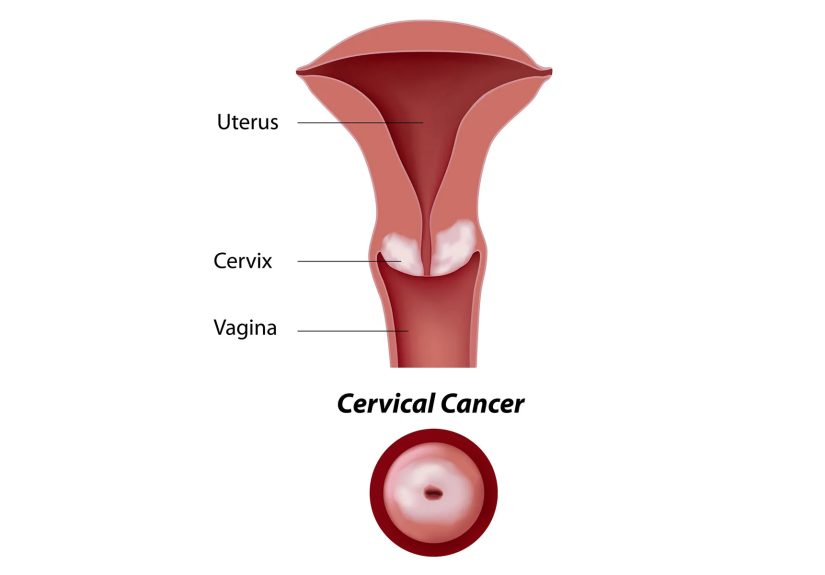
The cervix is the lower part of the uterus that connects to the vagina. Cervical cancer begins when cells in that area start growing out of control. Most cases are linked to a long-lasting infection with high-risk types of human papillomavirus, better known as HPV. That sounds intimidating, but it is also why prevention and early detection matter so much: there is a clear pathway from infection to abnormal cells to cancer, and modern medicine knows how to interrupt that journey.
This guide breaks down the symptoms, causes, risk factors, diagnosis, treatment options, and what the experience often feels like in real life. Because when it comes to cervical cancer, knowing the basics is not just helpful. It can be genuinely life-changing.
What Is Cervical Cancer?
Cervical cancer is a type of cancer that starts in the cervix. It usually develops over time rather than overnight. Before cancer appears, cervical cells often go through precancerous changes. These abnormal cells are not the same thing as cancer, but they can become cancer if they are not found and treated.
That slow progression is one reason cervical cancer screening is so valuable. Pap tests and HPV tests can detect abnormal changes or high-risk HPV before symptoms even show up. In other words, screening is not just a flashlight. It is sometimes a fire extinguisher.
Cervical Cancer Symptoms: What to Watch For
One of the trickiest things about cervical cancer symptoms is that early-stage disease may not cause any noticeable problems. A person can feel completely fine and still have abnormal cervical changes developing in the background. That is why screening matters even when everything seems normal.
Common symptoms of cervical cancer
- Abnormal vaginal bleeding, especially after sex
- Bleeding between periods
- Bleeding after menopause
- Unusual vaginal discharge, sometimes watery, bloody, or heavier than usual
- Pelvic pain
- Pain during sex
These symptoms do not automatically mean cancer. Infections, hormonal changes, benign growths, and other gynecologic conditions can cause similar issues. Still, this is not the moment for the old “I’ll just see if it goes away” routine. If bleeding, discharge, or pelvic pain feels unusual for you, it deserves medical attention.
Symptoms that may appear in more advanced disease
When cervical cancer becomes more advanced or returns after treatment, symptoms can expand beyond the cervix itself. Some people may experience pain in the abdomen, back, or leg, leg swelling, trouble urinating, changes in bowel habits, cough, or ongoing fatigue. These symptoms can have many causes, but they should never be brushed off as your body simply “being weird.” Your body is usually trying to send a message, not auditioning for improv comedy.
What Causes Cervical Cancer?
The main cause of cervical cancer is persistent infection with high-risk HPV. HPV is extremely common, and most sexually active people are exposed to it at some point. In many cases, the immune system clears the infection within a year or two. When high-risk HPV sticks around for years, however, it can trigger cell changes in the cervix that may progress to cancer.
Two high-risk HPV types, HPV 16 and HPV 18, are especially important because they account for a large share of cervical cancer cases. That does not mean every HPV infection turns into cancer. Most do not. But persistent high-risk HPV is the central driver of the disease.
This is also why HPV vaccination is such a major public health win. The vaccine does not treat an existing cancer, but it can help prevent infection with HPV types linked to cervical precancers and cancers. Prevention is not flashy, but it is powerful.
Risk Factors That Make Cervical Cancer More Likely
Having a risk factor does not mean someone will develop cervical cancer. It simply raises the odds. Some risk factors can be changed, while others cannot.
Major risk factors
- Persistent high-risk HPV infection: This is the biggest risk factor by far.
- Smoking: Tobacco use increases the risk and makes it harder for the body to clear HPV.
- Weakened immune system: Conditions such as HIV or medications that suppress immunity can reduce the body’s ability to control HPV.
- Lack of regular screening: When screening is skipped, precancerous changes are more likely to go unnoticed.
- Sexual history factors: More opportunities for HPV exposure can raise risk.
- Family history: A family history of cervical cancer may increase risk for some people.
- DES exposure before birth: This is less common today but still medically relevant for some families.
Some studies also associate long-term oral contraceptive use and multiple full-term pregnancies with a higher risk in certain groups. These factors are more complex and do not carry the same direct weight as persistent HPV infection, smoking, or missed screening.
How Cervical Cancer Is Diagnosed
If symptoms, screening results, or a pelvic exam raise concern, the next step is diagnostic testing. Doctors do not diagnose cervical cancer based on symptoms alone.
Tests used to diagnose cervical cancer
- Pelvic exam: A clinician checks for visible or physical abnormalities.
- Pap test: Looks for abnormal cervical cells.
- HPV test: Checks for high-risk HPV types.
- Colposcopy: Uses magnification to closely examine the cervix.
- Biopsy: Removes tissue so a pathologist can confirm whether cancer is present.
- Endocervical curettage: Samples tissue from the cervical canal when needed.
If cancer is confirmed, imaging and additional evaluation may be used to determine the stage. Staging helps show how far the cancer has spread and guides treatment decisions. In plain English, it answers the crucial question: “What exactly are we dealing with?”
Screening and Prevention: The Best Plot Twist
Even though this article focuses on symptoms, causes, and treatment, prevention deserves a starring role. Cervical cancer is one of the clearest examples in medicine of how prevention can dramatically change outcomes.
Screening recommendations people often hear in the U.S.
For many average-risk patients, U.S. guidance commonly includes Pap testing every 3 years from ages 21 to 29. From 30 to 65, screening may include primary HPV testing every 5 years, Pap testing every 3 years, or co-testing every 5 years, depending on clinical guidance and access. Screening plans can vary based on health history, prior abnormal results, immune status, and treatment history, so the right schedule should always be personalized.
Prevention strategies that actually matter
- Get the HPV vaccine if it is appropriate for your age and health history
- Keep up with routine cervical cancer screening
- Do not ignore abnormal bleeding or discharge
- Avoid smoking or get help quitting
- Follow up on abnormal Pap or HPV results instead of delaying care
A positive HPV test does not mean you have cancer. That point matters. It means follow-up is needed, not panic. The goal is to catch changes early, when treatment is simpler and outcomes are better.
Cervical Cancer Treatment: What the Options Look Like
Cervical cancer treatment depends on several factors, including the cancer stage, tumor size, lymph node involvement, overall health, and whether the patient wants to preserve fertility. There is no one-size-fits-all plan, and that is a good thing. Treatment is most effective when it matches the reality of the disease and the goals of the person being treated.
Treatment for very early changes and precancer
Not every serious cervical finding is invasive cancer. Some patients are treated for high-grade precancerous lesions before cancer develops. Procedures such as LEEP or cone biopsy can remove abnormal tissue and reduce the risk of progression. These treatments are often quick, effective, and far less disruptive than full cancer treatment.
Treatment for early-stage cervical cancer
When cancer is found early and remains confined to the cervix, surgery is often a major option.
- Radical hysterectomy: Removes the cervix, uterus, nearby tissue, and often nearby lymph nodes. This can be curative in many early-stage cases.
- Radical trachelectomy: Removes the cervix and surrounding tissue while leaving the uterus in place. In select early-stage cases, this may preserve the possibility of future pregnancy.
Fertility preservation is an important conversation, not a side note. For some patients with small, early-stage tumors, treatment can be designed with future family planning in mind. That does not make the decision easy, but it does make the conversation essential.
Treatment for locally advanced cervical cancer
For larger tumors or cancer that has spread beyond the cervix but remains in the pelvis, the standard approach is often chemoradiation. This typically combines external-beam radiation therapy, brachytherapy, and cisplatin-based chemotherapy given at the same time.
Brachytherapy deserves special mention because it is a cornerstone of treatment for many cervical cancers. It places radiation close to the tumor area, allowing a strong local effect while limiting damage to surrounding tissue. It may not sound glamorous, but in oncology, “precise and effective” beats glamorous every single time.
Treatment for advanced, recurrent, or higher-risk disease
When cervical cancer is more advanced, has spread, or comes back after initial treatment, therapy may include systemic treatment such as chemotherapy, immunotherapy, or a combination approach. In some settings, pembrolizumab has become part of treatment alongside chemoradiation for certain higher-risk patients, reflecting how fast cancer care continues to evolve.
Some patients may also be candidates for clinical trials, which can offer access to promising new therapies. For recurrent or metastatic disease, treatment goals may include controlling the cancer, reducing symptoms, improving quality of life, and extending survival.
Side Effects and Recovery: The Part Nobody Should Sugarcoat
Cervical cancer treatment can be highly effective, but it is not effortless. Surgery may affect fertility, menopause timing, bladder function, bowel function, and sexual health. Radiation can cause fatigue, bowel changes, bladder irritation, vaginal changes, and long-term pelvic effects. Chemotherapy may bring nausea, blood count changes, neuropathy, and exhaustion that feels less like “being tired” and more like your battery has filed for permanent leave.
This is why supportive care matters so much. Pain control, nutrition support, pelvic floor therapy, sexual health counseling, mental health care, and practical help with transportation or work leave are not extras. They are part of real cancer care.
What Prognosis Depends On
Prognosis depends on the stage at diagnosis, tumor characteristics, response to treatment, and overall health. In general, cervical cancer found early is much more treatable than cancer found late. That is one more reason regular screening is such a big deal. It can lead to earlier detection, less aggressive treatment, and better odds of long-term survival and quality of life.
When to See a Doctor
Make an appointment if you notice vaginal bleeding after sex, between periods, or after menopause; unusual discharge; pelvic pain; or pain during sex. Also seek follow-up if you have an abnormal Pap or HPV result, even if you feel perfectly fine. “No symptoms” does not always mean “no problem.”
If you have already been diagnosed, ask direct questions: What stage is it? What are my treatment options? Can fertility be preserved? What side effects should I expect? Is a gynecologic oncologist involved? Good cancer care includes good explanations.
Real-Life Experiences With Cervical Cancer: What Many Patients Go Through
Beyond the clinical language, cervical cancer is often experienced as a series of emotional whiplash moments. Many patients describe the diagnosis starting with something they almost ignored: light bleeding after sex, spotting that seemed random, a Pap test they expected to be routine, or an HPV result that sounded scary before anyone had explained what it really meant. A lot of people say the hardest part in the beginning is uncertainty. They are not yet thinking about treatment plans or staging details. They are thinking, “How serious is this?” and “What happens next?”
Another common experience is guilt, especially when HPV enters the conversation. Some patients unfairly blame themselves, even though HPV is incredibly common and often silent. Others feel embarrassed discussing symptoms or sexual history, which can delay care. That emotional burden is real, and it is one reason compassionate, stigma-free communication matters so much. Nobody should feel shamed while trying to get cancer care.
Patients with early-stage disease often describe a strange mix of relief and fear. Relief, because the cancer was caught early. Fear, because even “good news” in cancer still includes words like biopsy, surgery, and follow-up surveillance. Those pursuing fertility-sparing treatment may face especially difficult decisions. They are not only weighing cancer control. They may also be grieving possible changes to future family plans while trying to stay calm in exam rooms that smell faintly of antiseptic and big decisions.
People going through chemoradiation often talk about how treatment becomes its own full-time rhythm. Appointments pile up. Fatigue becomes more than ordinary tiredness. Some say the physical symptoms are manageable compared with the mental grind of repeated visits, waiting for results, and trying to act normal while life suddenly revolves around oncology calendars. Support from partners, friends, family, or other survivors can make a major difference. So can practical help: rides, meals, child care, and someone who remembers the questions you forgot to ask.
Survivorship brings its own adjustment period. Many patients feel grateful, but not instantly carefree. Follow-up scans and exams can trigger anxiety. Some deal with long-term effects on sexual health, menopause symptoms, body image, or fertility. Others become passionate about reminding friends and relatives not to skip screening. In that sense, cervical cancer often changes how people think about routine care. Pap tests stop feeling optional. HPV vaccination stops sounding abstract. The experience can be frightening, but it also makes one truth impossible to ignore: early attention saves people from harder roads later.
Conclusion
Cervical cancer is serious, but it is not invisible and it is not unbeatable. Persistent high-risk HPV is the main cause, symptoms often involve abnormal bleeding or discharge, and treatment can range from minor procedures for precancer to surgery, chemoradiation, and newer systemic therapies for more advanced disease. The most important takeaway is simple: do not wait for dramatic symptoms. Keep up with screening, follow up on abnormal results, and take unusual bleeding seriously. Sometimes the best cancer strategy is not heroic. It is timely, informed, and stubbornly proactive.





